

The kids finish school this week. The last day for the district is Friday. We had only one or two snow days this year so they will finish as scheduled, unlike the last few years. Lilly’s last day is Friday. Shawn will finish on Thursday since he’ll be in surgery at CHOP on Friday. He missed the last day of school and the first day of school. In between those those days was an unusual first grade experience.
Lilly is “graduating” from fifth grade. No more elementary school for her. As of Saturday, she will be a Middle Schooler (god help us all!) although the kids call the time in between grades “summer grade” rather than placing themselves in the next higher grade, like I eagerly did when I was a kid.
Shawn is finishing first grade. Well, sorta. Shawn didn’t attend more of first grade than he did attend. I lost count and can’t easily look it up but I estimate that out of 180 days that the kids were supposed to be AT school,

Shawn missed at least 100 of them. Probably more. But in late May, sitting on the floor in our living room with his home-instruction teacher, Miss Johnson, Shawn officially completed the assessments that indicate that he knows what a first grader in our school district is expected to know. I admit, I’d been concerned about this. Shawn had been a smart and interested but average student throughout preschool and kindergarten. He wasn’t “advanced”. This stuff doesn’t come naturally to him. He needs help to learn. He needs school. And he wasn’t there more than he was there. There were weeks that went by that he didn’t even brush his teeth or eat, let alone do anything academic. But here he is, finishing first grade.
In retrospect, Shawn’s earliest obvious symptoms showed up the first week of summer vacation last year. I took a week off from work to hang out with the kids and on Monday we set off to explore caves and coal mines in central Pennsylvania but Shawn got sick in the car while getting gas and breakfast less than a mile from the start. We went back home. The first of a series of “car sicknesses” and “stomach bugs” that would follow him throughout the summer. The vomiting that in mid August would still cause me to say “at least we’re getting the sickness out of the way before school starts in a couple weeks” and eventually take him to his pediatrician by the end of the month because something seemed really wrong by then. By the second week of the school year, we’d begun our CHOP adventures. It would be almost seven more months until we figured out what was actually wrong. Shawn would become very angry during those months. He would respond well to only one category of CHOP people – his teachers.
As the admissions piled up in September and October, I diligently called the school to report each absence and sent in the Discharge Papers and the Return To School notes signed by a doctor. I always asked to pick up Shawn’s homework with the intent of keeping him on target with what his class was learning. Maybe not all the way but as best as we could when he was feeling ok. We practiced spelling words and did math problems and read books from the play room on 9 South when he was feeling ok.
One day while I was out running at CHOP in October, I got a phone call from his school. His homeroom teacher, Mrs. Klein, and principal, Mrs. Gregitis, were calling to discuss a more long term plan, the kind that they create for kids who are out for extended periods of time. I slowed to a walk and talked with them. “Don’t worry about the homework,” they said, “it’s intended to reinforce what’s being taught in the classroom and he’s not IN the classroom.” They gave me some things to focus on instead. We initiated the process to start hospital instruction.
Later that month, during Shawn’s longest straight admission, he began working with a hospital teacher, Ryan. For the first time at CHOP, Shawn was engaged, responsive and happy. He looked forward to each day’s hour with her. She told us how wonderful it was to work with our school district, how responsive they were. When we went back to CHOP inpatient in January, I was disappointed to find out that Maria would be our new teacher, not Ryan, since Shawn liked Ryan so much and he responds best to people he already knows. But he instantly loved Maria, too. He loved all his teachers and I began looking forward to it as the time that Shawn would be happy. When Shawn refused to cooperate with the doctors, I told them that if they want to watch Shawn’s speech, movements, and behavior, come watch him when he’s with his teacher. They’ll see everything they are looking for.
For the first time at CHOP, Shawn was engaged, responsive and happy. He looked forward to each day’s hour with her. She told us how wonderful it was to work with our school district, how responsive they were. When we went back to CHOP inpatient in January, I was disappointed to find out that Maria would be our new teacher, not Ryan, since Shawn liked Ryan so much and he responds best to people he already knows. But he instantly loved Maria, too. He loved all his teachers and I began looking forward to it as the time that Shawn would be happy. When Shawn refused to cooperate with the doctors, I told them that if they want to watch Shawn’s speech, movements, and behavior, come watch him when he’s with his teacher. They’ll see everything they are looking for.

")
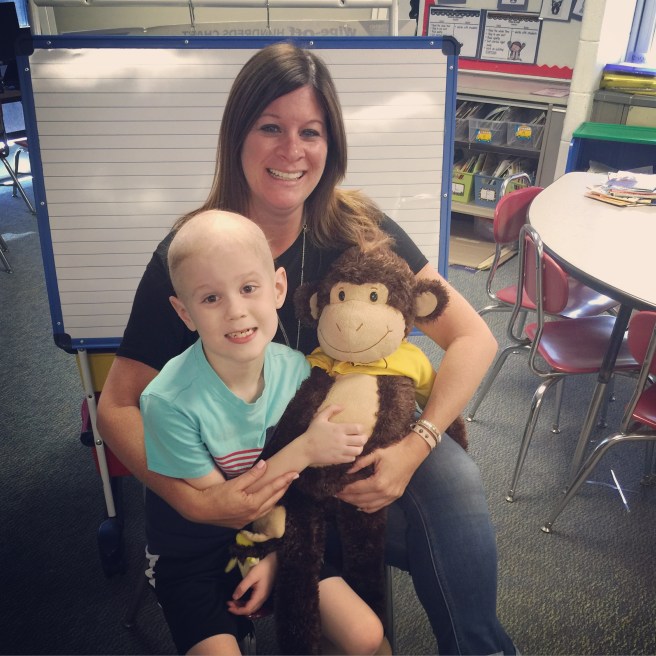
By March we knew that the root of his problems was cancer. A cancer diagnosis opens a lot of doors for a sick kid that being undiagnosed does not. One of the social workers asked if Shawn might be interested in the Monkey In My Chair program. When we explained to Shawn that it means that a big stuffed monkey would sit in his seat at school when he wasn’t there, he excitedly said yes! The monkey came in the mail a couple weeks later. Shawn named him Happy.
It was a terrible year filled with numerous hospital stays, a lot of pain and sickness, and, well, eventually a cancer diagnosis. Childhood probably doesn’t get much shittier than all of that. But other than his family, his teachers were the people he loved the most throughout this year. Even when he pretty much hated everyone else.




















 I can’t say that I’m not scared shitless about this process. I can’t even say anything positive about it other than that I hope it works. But today was a good day. I don’t know what tomorrow will be but today turned out ok.
I can’t say that I’m not scared shitless about this process. I can’t even say anything positive about it other than that I hope it works. But today was a good day. I don’t know what tomorrow will be but today turned out ok.







